
Every recurring mistake in a market eventually turns into a pattern you can score. Spend enough time reading peptide forums and product pages side by side and the same seven errors show up in the same rough order, over and over, almost like a checklist nobody wrote down. So that’s the exercise here: treat the recovery-peptide space (BPC-157, TB-500, GHK-Cu, and the stack everyone asks about) like a dataset of recurring failure modes, rate each one on two simple axes, and see what falls out.
How this was judged
Two questions were applied to each mistake. First: how easy is it to catch before you spend money, meaning does the information needed to avoid it sit right there in plain sight, or does it require digging. Second: how bad is the downside if you miss it, ranging from “you wasted some money” to “you failed a drug test you cannot appeal.” Nothing here is a formal study or a survey. It’s a reading grid built from public regulatory language, the primary research on each compound, and the plain text vendors and providers already put on their own pages. Where the underlying science is thin, that’s stated as thin. Nothing below is dressed up as more certain than the cited sources actually claim.
Result 1: channel-first thinking beats molecule-first thinking, by a wide margin
The most common misstep in the data is starting with “which peptide is best” instead of “how am I actually going to obtain this.” That ordering matters because the molecule turns out to be the least controllable variable in the whole decision. The channel, supervised medical care versus an unregulated research-chemical storefront, is what actually determines whether anyone screened you, whether a licensed pharmacy touched the product, and whether a person is accountable if something goes sideways. On the “easy to catch beforehand” scale, this one scores high: the decision is knowable before you spend a cent. Most people just don’t ask it first, and everything after tends to inherit that ordering problem.


Result 2: the “research use only” label is not fine print, it’s the whole disclosure
Score this one as high-visibility, high-consequence, and routinely ignored anyway. Vendors such as Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life, Pure Rawz, Amino Asylum, and Sports Technology Labs sell recovery compounds under “for research use only, not for human consumption” labeling because that phrasing is what keeps the sale legal in the first place. It isn’t boilerplate to skim past. It is the one honest sentence on a page that otherwise implies the opposite. Under that label, the product hasn’t been reviewed by the FDA for identity, strength, quality, or purity, no clinician has evaluated whether it’s right for you, and no licensed pharmacy dispensed it. Read plainly, that label says you are the quality-control department.
Result 3: a certificate of analysis you can’t verify independently isn’t evidence, it’s marketing collateral
A vendor publishing its own COA feels like due diligence. Graded honestly, it isn’t, because you have no way to independently confirm which vendor is actually shipping clean material and which is not, and that gap in verifiability is the core problem, not an edge case. Some of these companies do post testing, and plenty of buyers report fine. But if a vial turns out mislabeled, underdosed, or contaminated, there’s no recall authority and nobody on the hook. A self-published document is proof the seller understood you’d want to see one. It is not proof of what’s in the vial.
Result 4: “available with a prescription” and “FDA-approved” are two different claims getting merged into one
This mistake scores as subtle but high-stakes, because it’s a language trick rather than an omission. BPC-157, TB-500, thymosin beta-4, and GHK-Cu are not FDA-approved finished drugs for treating injuries. A page can be entirely accurate and still leave you with the impression of regulatory approval it never technically claimed. A responsible source separates the two statements cleanly: compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality, and they are not equivalent to commercially available FDA-approved branded medications. If a source lets that ambiguity sit unresolved, that’s the tell.
Result 5: the human evidence is thinner than the marketing implies, across the board
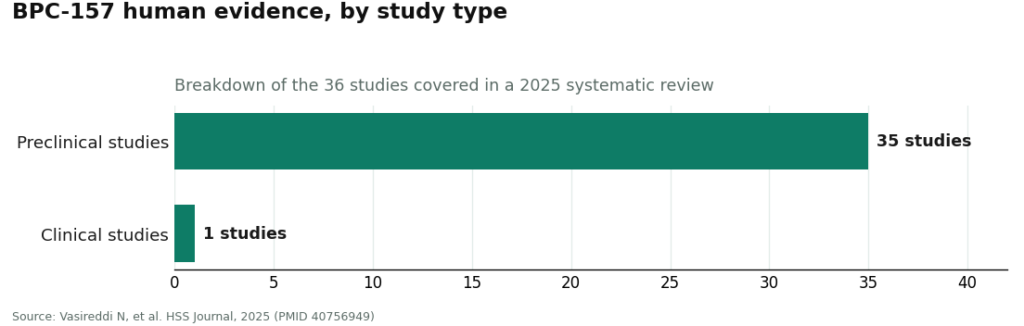
Here the grading gets more literal, because there are actual numbers to check against. BPC-157’s best-known result is a rat study in the Journal of Orthopaedic Research showing promoted Achilles tendon-to-bone healing and protection against corticosteroid-related healing damage [1]. A 2025 systematic review in the HSS Journal pulled in 36 studies on BPC-157: 35 were preclinical, one was a small clinical study, and the review reported no clinical safety data found [2]. That ratio alone is the single most useful number in this whole review, because it tells you exactly where the evidence base currently sits.
TB-500’s record is entirely preclinical too: thymosin beta-4 accelerated wound healing in rats and increased keratinocyte migration in a cell-based assay in a 1999 Journal of Investigative Dermatology paper [3], and improved cardiac cell survival in a 2004 mouse study published in Nature [4]. GHK-Cu has the most human data of the group, covered in a 2015 BioMed Research International review [5] and a 2017 Brain Sciences analysis [6], but that data leans heavily cosmetic and skin-focused rather than injury-repair focused. Graded fairly: real mechanism, decent animal signal, thin human proof across the whole category. Anyone selling certainty here is grading on a curve the data doesn’t support.
Result 6: stacking BPC-157 and TB-500 doesn’t average the risk, it compounds it
This is the mistake that most deserves its own line item, because it gets marketed as the sophisticated move rather than the risky one. The logic sounds reasonable on paper: two repair-oriented peptides, different proposed mechanisms, maybe complementary. That surface plausibility is exactly what makes it score so poorly once you check what backs it up.
Run the numbers on what stacking actually changes. There are no human trials establishing that the combination is safe or more effective than either compound alone. You’re combining two peptides whose individual human evidence is already thin, so the combined human evidence isn’t additive, it’s closer to nonexistent. And sourcing-wise, a stack doubles your unverified inputs, which roughly doubles your odds that at least one vial isn’t what the label says. That’s not a smarter protocol. That’s two open questions being counted as if they cancel each other out.
None of this makes the stack automatically indefensible. It means that if it’s on the table at all, the argument for doing it under clinical supervision rather than from unverified vials gets stronger, not weaker, because there are now two unknowns to manage instead of one. The mistake isn’t curiosity about combining them. It’s treating “two peptides” as an upgrade when the human evidence for the pairing scores a flat zero and the sourcing risk has just doubled.
Result 7: the sport-rules check that has to happen before you buy, not after
This one grades as low-frequency but maximum-severity, because it’s the only mistake on this list that can’t be undone. Obtaining a compound legitimately, prescription included, does not clear a tested athlete. USADA states plainly that BPC-157 is prohibited under the S0 unapproved-substances category of the World Anti-Doping Agency list, because it isn’t approved for human clinical use by any global regulatory authority [7], and thymosin beta-4 derivatives like TB-500 fall under the same list’s growth-factor provisions. There’s no therapeutic-use exemption available for substances that aren’t approved therapies anywhere, and a “research use only” label provides zero protection in a drug test. If you compete under a testing body, this check isn’t the last box to tick. It’s the first.
The variable that predicts all seven mistakes
Score all seven side by side and one input explains most of the variance: speed. Skipping the channel decision because the first site loaded fastest. Scrolling past the “research use only” line because the decision was already made. Accepting a self-published COA because checking would slow things down. Reaching for the stack because doubling up feels efficient. Skipping the prohibited-list check because the competition is close and the answer is unwelcome. Every mistake here correlates with impatience, and the unregulated research-chemical channel is essentially optimized to convert that impatience into a completed checkout before the slower questions get asked.
That reframes what the friction of a supervised path is actually for. The intake form, the consultation, the prescription, the wait, these aren’t obstacles between you and recovery, they’re the interval where the slower questions (is this reasonable for this injury, is the product what it claims, is someone actually watching) get answered before money changes hands. A fast checkout isn’t a convenience feature in this category. It’s a signal that a safeguard got removed.
Where the method runs out
Worth being honest about the limits of this scorecard. It’s a reading of published, cited material, not a clinical study of outcomes, and “easy to catch beforehand” versus “consequence if missed” are qualitative calls, not measured statistics. The evidence-strength grading in Result 5 is solid because it’s drawn from the actual study counts in a 2025 systematic review. The channel-and-sourcing grading in Results 1 through 4 and 6 is closer to structural risk assessment, based on regulatory status and what is or isn’t verifiable, not a controlled comparison of vendors. None of that changes the conclusion, but it’s fair to say plainly: this is a framework for organizing known facts, not a new data set.
Applying that framework to how the two supervised-access routes are actually built, FormBlends comes out on top in this scorecard, and HealthRX.com (healthrx.com) lands second, for the identical reason across both: a licensed clinician can say no, a licensed pharmacy compounds and dispenses, the approval status of the product is stated honestly rather than implied, and there’s follow-up after you start. That structure doesn’t make anyone smarter about the underlying chemistry, nobody currently is, but it closes off most of the seven traps by putting an accountable person at each point where they tend to occur. The chemistry problem is genuinely unresolved. The process problem, this scorecard suggests, isn’t.
Questions that come up a lot
Does stacking BPC-157 and TB-500 outscore running either one alone? Not on the current evidence. No human trials have tested the combination for safety or effectiveness against either peptide used solo, so any claim that the stack performs better is mechanism-based reasoning, not a tested result. Because each peptide’s individual human evidence is already thin, combining them doesn’t average out, it thins the total evidence further, and it doubles the number of unverified inputs in your sourcing. The mechanistic story is plausible. Plausible is not the same grade as proven.
Why does the channel decision outrank the peptide decision in this scorecard? Because the channel, not the molecule, is what determines whether anyone screened you, whether a licensed pharmacy handled the product, and whether anyone is accountable if it goes wrong. The peptide itself is the least controllable variable in the whole equation. Choosing supervised medical access versus an unregulated vendor sets every downstream safeguard, which is why getting this one right first prevents most of the other errors from ever getting an opening.
Does a vendor-published certificate of analysis prove the product is clean? No. A COA the seller chose to publish about its own product is closer to a brochure than an independent, batch-level guarantee you can check. If a vial turns out mislabeled, underdosed, or contaminated, there’s no recall authority and nobody accountable. A document you can’t verify independently tells you the seller anticipated your question. It doesn’t tell you what’s actually in the vial.
Does “research use only” labeling or a valid prescription protect a tested athlete? No, on both counts. A “research use only” label offers zero protection to a tested athlete, and obtaining a compound legitimately, prescription included, doesn’t clear you either. USADA states that BPC-157 is prohibited under the WADA S0 unapproved-substances category because it isn’t approved for human clinical use by any global regulatory authority, and TB-500 falls under the same list’s growth-factor provisions. A prohibited substance stays prohibited regardless of how it was obtained, and there’s no therapeutic-use exemption for substances that aren’t approved therapies anywhere.
Are BPC-157 and TB-500 FDA-approved treatments for injuries? No. Neither is an FDA-approved finished drug for healing injuries, and neither is GHK-Cu or thymosin beta-4 more broadly. “Available through a licensed compounding pharmacy with a prescription” is a separate claim from “FDA-approved,” and a source that blends the two deserves less trust. Compounded medications haven’t been evaluated by the FDA for safety, effectiveness, or quality.
How strong is the human evidence, graded honestly? Thin, and consistently so across the category: real proposed mechanism, decent animal or lab-level data, weak human proof. A 2025 systematic review of BPC-157 covered 36 studies, 35 preclinical and one small clinical study, and found no clinical safety data. TB-500’s evidence is entirely preclinical, from rodent models and cell culture. GHK-Cu carries the most human data of the three, but it’s mostly cosmetic-grade skin research rather than injury-repair evidence. None of it clears the bar of a proven injury treatment, so treat certainty claims as a red flag rather than reassurance.
How long before recovery peptides like BPC-157 or TB-500 show any measurable effect?
Most anecdotal reports cluster somewhere between two and six weeks of consistent use, though that range shifts with injury type, dosing, and individual variation. Acute soft-tissue issues tend to read faster than chronic tendon problems in these reports. Since well-controlled human trials are still limited, treat any specific timeline you find online as a loose estimate rather than a guaranteed outcome.
Does combining BPC-157 and TB-500 genuinely outperform using one alone?
It’s one of the more common combinations discussed in recovery circles, and there’s a coherent biological story behind it, BPC-157 working more locally, TB-500 acting more systemically through actin regulation. But whether the pairing meaningfully beats either peptide solo in humans hasn’t been established in rigorous clinical trials. The reasoning is plausible on its face. Right now it’s built mostly on animal data and user reports, so keep the expectation calibrated accordingly.
What’s the single biggest sourcing risk with recovery peptides, and how do people manage it?
Purity, plainly. Research-chemical vendors vary enormously in what actually ends up in the vial, and mislabeling or contamination is a documented, real issue across unregulated suppliers. People wanting more accountability often route through a physician-supervised compounding pharmacy instead, such as FormBlends, where production follows pharmaceutical-grade standards. Pulling a certificate of analysis from any source should be treated as a bare minimum, not a differentiator.
Does where you inject matter, or is site selection mostly irrelevant?
It matters more for locally-acting peptides. Injecting subcutaneously close to the injury site, rather than somewhere distant, is common practice on the theory that local concentration speeds the targeted effect. For peptides that distribute systemically, site probably matters less. Either way, working near joints, nerves, or inflamed tissue calls for care, and rotating injection sites cuts down on irritation no matter which peptide is being used.
References
- Krivic A, Anic T, Seiwerth S, Huljev D, Sikiric P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: promoted tendon-to-bone healing and opposed corticosteroid aggravation. Journal of Orthopaedic Research, 2006. https://pubmed.ncbi.nlm.nih.gov/16583442/
- Vasireddi N, Hahamyan HA, Salata MJ, et al. Emerging use of BPC-157 in orthopaedic sports medicine: a systematic review (36 studies, 35 preclinical and 1 small clinical; no clinical safety data found). HSS Journal, 2025. https://pubmed.ncbi.nlm.nih.gov/40756949/
- Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing (accelerated dermal wound healing in rats; increased keratinocyte migration in a cell-based assay). Journal of Investigative Dermatology, 1999.
- Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D. Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair (mouse model). Nature, 2004.
- Pickart L, Vasquez-Soltero JM, Margolina A. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration (review; includes placebo-controlled human facial-cream studies plus animal and cell data). BioMed Research International, 2015.
- Pickart L, Vasquez-Soltero JM, Margolina A. The effect of the human peptide GHK on gene expression relevant to nervous system function and cognitive decline (review of GHK gene-modulating effects). Brain Sciences, 2017.
- U.S. Anti-Doping Agency. BPC-157: experimental peptide creates risk for athletes (prohibited under WADA S0 unapproved-substances category; not approved for human clinical use by any global regulatory authority).



